
The Anesthesia Gas Machine 2026
Michael P. Dosch PhD CRNA (ret), Darin Tharp CRNA MS
University of Detroit Mercy - Nurse Anesthesia
This site is https://healthprofessions.udmercy.edu/academics/na/agm/.
Revised Feb. 2026
The Anesthesia Gas Machine 2026
Michael P. Dosch PhD CRNA (ret), Darin Tharp CRNA MS
University of Detroit Mercy - Nurse Anesthesia
This site is https://healthprofessions.udmercy.edu/academics/na/agm/.
Revised Feb. 2026
Dry gas supplied by the gas machine may cause clinically significant desiccation of mucus and an impaired mucociliary elevator. This may contribute to retention of secretions, blocking of conducting airways, atelectasis, bacterial colonization, and pneumonia.
Some examples:
It is ideal to provide gases at body temperature and 100% RH to the patient’s airway. For cases lasting longer than 1 hour, humidification measures are often employed including:
The heat and moisture exchanger has large thermal capacity, hygroscopic, and (sometimes) bacterial filtration. It can do no more than return the patient’s exhaled water- it can’t add heat or moisture- and it is less efficient with longer cases or higher flows. But it’s easy to use, inexpensive, silent, won’t overheat or overhydrate the patient.
FGF determines not just FIO2, but also the speed with which you can change the composition of gases in the breathing circuit.
Low flows are used to decrease the usage, cost, and pollution of volatile anesthetics. A 50% reduction in FGF translates to a 50% savings on gaseous anesthetic agent, without placing the patient at risk or lessening the quality of their care (savings are offset by quicker consumption of absorbent). Tracheal heat and humidity, and patient core body temperature are preserved better than at higher flows. Low flows are ecologically sound, lessening the release of volatile agents and nitrous oxide, with their global warming potential. [3]
The composition of gases in the breathing circuit may change as lower flows are employed, since a greater fraction of the gas inspired by the patient will be rebreathed.

|
Car heater controls- fan and heat mix. Click on the link to see the larger version. |
Large discrepancies between dialed and inspired agent concentration can be unsettling, raising apprehensions about vaporizer or breathing circuit malfunction. An analogy may help to clarify why this is an expected result of low flows.
Imagine you are entering an automobile in the winter. You turn the heater on at maximum heat level and fan speed. After the car is warmed to a comfortable temperature, you can't turn the heater entirely off. Heat must still be supplied, since it is always escaping (the car is not airtight). To keep the car at the desired temperature, you may either a) flow a moderate to high fan speed, but decrease the heat mix to nearly room temperature air, or b) you may leave the heat mix level high, and slowly blow in a small amount of very hot air. It makes no difference- in either case the car stays at the desired temperature.
Similarly, we begin cases with higher flows. Since there is little rebreathing at 4 L/min FGF and above, the dialed and inspired agent concentration are very similar. We induce with overpressure until the patient is saturated (reflected in an end-tidal agent concentration which closely approaches inspired). Then we may either a) leave the flows high with a moderate agent concentration near MAC, or b) turn the flows to low flow. But if we use low flows, we must still provide the same number of molecules of agent in order to replace that lost due to dilution, leaks, and uptake to fat and muscle. So with low FGF, we must turn the vaporizer dial beyond what we might have at higher flows.
There are two excellent comprehensive reviews of low flow anesthesia noted below.[12], [13]
You can "preoxygenate" with a nasal cannula or any other oxygen source. We need to do more- denitrogenate (cleanse the functional residual capacity of nitrogen)- to help our patients tolerate a potential period of apnea (if we have difficulties with intubation).
Clinical presentation The cause of the symtoms (tachycardia, tachypnea, and elevated end-tidal CO2) seen in malignant hyperthermia (MH) must be distinguished from ventilator or unidirectional valve malfunctions (producing respiratory acidosis), hyperthyroidism, cocaine intoxication, pheochromocytoma, and sepsis.
Triggers Succinylcholine and all inhaled agents are the only anesthetic agents that will trigger MH.
Treatment of acute episodes in OR High fresh gas flow (10 L/min), notify surgeon, hyperventilation, use activated charcoal filters on inspiratory and expiratory limbs of breathing circuit, stop inhaled agents and remove vaporizers, stop succinylcholine, and as time permits change soda lime granules & breathing circuit. The mainstay of treatment is dantrolene 2.5 mg/kg (up to 10 mg/kg). Cooling by any and all means, NaHCO3, treatment of hyperkalemia, and other measures are also important. MHAUS (Malignant Hyperthermia Association of the US) publishes lists of recommendations for management of acute crisis at MHAUS.org.
Management of known susceptible patients- MHAUS recommends four alternatives to prepare the gas machine:
Most common site is Y piece. The most common preventable equipment-related cause of mishaps. Direct your vigilance here by:
Beside inability to ventilate, obstruction may also lead to barotrauma. Obstruction may be related to:
Much less of a problem since breathing circuit and scavenger tubing sizes have been standardized. However, breathing systems are reconfigured for preventive maintenance and other reasons. One such incident resulted in apnea, inability to ventilate, and cardiac arrest (asystole) in 2007. [21]
May be due to failure to check cylinder contents, or driving a ventilator with cylinders when the pipeline is unavailable. This leads to their rapid depletion, perhaps in as little as an hour, since you need approximately a VT of driving gas per breath, substantially more if airway resistance (RAW) is increased. [22]
Clean the bellows after any patient with diseases which may be spread through airborne droplets, or don’t use the mechanical ventilator, or use bacterial filters, or use disposable soda lime assembly, or use a Bain.
Protocol for mechanical ventilator failure
|
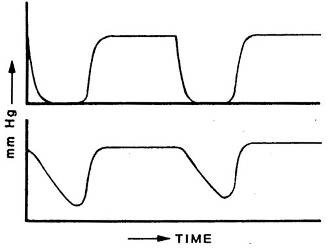
Inspired unidirectional valve problem- bottom capnogram. Click on the link to see the larger version. The causes of increased inspired carbon dioxide are almost exclusively either malfunctioning unidirectional valves, or exhausted absorbent. |
Increased inspired carbon dioxide has other potential causes, but these are rare
Many treatment approaches waste precious time: increasing minute ventilation; seeking signs of malignant hyperthermia; checking for leaks in the circuit; obtaining arterial blood gases; performing bronchoscopy for mucous plugs; inserting central lines; recalibrating or replacing ventilator, capnograph, or the entire gas machine.
Malfunctioning unidirectional valves can cause serious problems.
Increased carbon dioxide production will not result in increased inspired carbon dioxide. The capacity of the soda lime granules is sufficient to cleanse each breath entirely, even if carbon dioxide production is increased. Further, respiratory acidosis will not cause visibly dark blood, or desaturation on the pulse oximeter.
(Absent the rare causes mentioned above) if the granules are not exhausted, and the inspiratory and expiratory unidirectional valves are forcing all exhaled gas through the granules, there can be no increase in inspired carbon dioxide. So, if it is detected:
[1] Dosch MP, Loeb RG, Brainerd TL, Stallwood JF, Lechner S. Time to a 90% change in gas concentration: a comparison of three semi-closed anesthesia breathing systems. Anesth Analg. 2009 Apr;108(4):1193-7. doi: 10.1213/ane.0b013e3181949afd.
[2] Kennedy RR, Hendrickx JF, Feldman JM. There are no dragons: Low-flow anaesthesia with sevoflurane is safe. Anaesth Intensive Care. 2019 May;47(3):223-225. doi: 10.1177/0310057X19843304.
[3] ASA Committee on Equipment and Facilities (2023). Statement on the Use of Low Gas Flows for Sevoflurane. https://www.asahq.org/standards-and-practice-parameters/statement-on-the-use-of-low-gas-flows-for-sevoflurane, Accessed Feb 2, 2026
[4] Varughese S, Ahmed R. Environmental and Occupational Considerations of Anesthesia: A Narrative Review and Update. Anesth Analg. 2021 Oct 1;133(4):826-835. doi: 10.1213/ANE.0000000000005504.
[5] De Cooman S, Schollaert C, Hendrickx JF, Peyton PJ, Van Zundert T, De Wolf AM. Hypoxic guard systems do not prevent rapid hypoxic inspired mixture formation. J Clin Monit Comput. 2015 Aug;29(4):491-7. doi: 10.1007/s10877-014-9626-y. (especially video content)
[6] Eriksson S, Sixten B. More on the danger of inhaling air at reduced fresh gas flows: a self-experiment. J Clin Monit Comput. 2016 Apr;30(2):251-2. doi: 10.1007/s10877-015-9710-y.
[7] Ghijselings IE, De Cooman S, Carette R, Peyton PJ, De Wolf AM, Hendrickx JF. Performance of an active inspired hypoxic guard. J Clin Monit Comput. 2016 Feb;30(1):63-8. doi: 10.1007/s10877-015-9684-9.
[8] Wetz AJ, Mueller MM, Walliser K, Foest C, Wand S, Brandes IF, Waeschle RM, Bauer M. End-tidal control vs. manually controlled minimal-flow anesthesia: a prospective comparative trial. Acta Anaesthesiol Scand. 2017 Nov;61(10):1262-1269. doi: 10.1111/aas.12961.
[9] Singaravelu S, Barclay P. Automated control of end-tidal inhalation anaesthetic concentration using the GE Aisys Carestation™. Br J Anaesth. 2013 Apr;110(4):561-6. doi: 10.1093/bja/aes464.
[10] Getinge 2025. https://www.getinge.com/int/products-and-solutions/operating-room/anesthesia/AGC/ Accessed Feb 2, 2026
[11] Serefoglu R, Kocayigit H, Palabiyik O, Tuna AT. Comparison of automated and manual control methods in minimal flow anesthesia. J Clin Monit Comput. 2024 Oct;38(5):1117-1123. doi: 10.1007/s10877-024-01163-0.
[12] Hönemann C, Hagemann O, Doll D. Inhalational anaesthesia with low fresh gas flow. Indian J Anaesth. 2013 Jul;57(4):345-50. doi: 10.4103/0019-5049.118569.
[13] Honemann C, Mierke B. Low-flow, minimal-flow and metabolic-flow anaesthesia: Clinical techniques for use with rebreathing systems. 2015:Dräger (see page 86 for discussion of contraindications) at https://www.draeger.com/Content/Documents/Content/low-minimal-flow-anaesthesie-bk-9067990-en-global.pdf Accessed Feb 2, 2026
[14] Benumof JL. Preoxygenation: best method for both efficacy and efficiency. Anesthesiology. 1999 Sep;91(3):603-5. doi: 10.1097/00000542-199909000-00006.
[15] Malignant Hyperthermia Association of the US. Safe and Unsafe Anesthetics. https://www.mhaus.org/healthcare-professionals/be-prepared/safe-and-unsafe-anesthetics/ Accessed Feb , 2026
[16] Kim TW, Nemergut ME. Preparation of modern anesthesia workstations for malignant hyperthermia-susceptible patients: a review of past and present practice. Anesthesiology. 2011 Jan;114(1):205-12. doi: 10.1097/ALN.0b013e3181ee2cb7.
[17] Boriosi JP, Hollman GA. Making a case for use of the pretracheal stethoscope in pediatric procedural sedation. Paediatr Anaesth. 2016 Mar;26(3):249-55. doi: 10.1111/pan.12849.
[18] Fisher QA. Can capnography substitute for auscultation in sedation cases? Anesth Analg. 2005 May;100(5):1546. doi: 10.1213/01.ANE.0000151470.50760.4A.
[19] Lofsky AS. Turn Your Alarms On! APSF Newsl 2004. https://www.apsf.org/article/turn-your-alarms-on/ Accessed Feb 2, 2026
[20] Mehta SP, Eisenkraft JB, Posner KL, Domino KB. Patient injuries from anesthesia gas delivery equipment: a closed claims update. Anesthesiology. 2013 Oct;119(4):788-95. doi: 10.1097/ALN.0b013e3182a10b5e.
[21] US FDA. Adverse event report MW5003097, Manufacturer and User Facility Device Experience [MAUDE] database, 2007
[22] Taenzer AH, Kovatsis PG, Raessler KL. E-cylinder-powered mechanical ventilation may adversely impact anesthetic management and efficiency. Anesth Analg. 2002 Jul;95(1):148-50, table of contents. doi: 10.1097/00000539-200207000-00026.
[23] Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, Fiadjoe JE, Greif R, Klock PA, Mercier D, Myatra SN, O'Sullivan EP, Rosenblatt WH, Sorbello M, Tung A. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022 Jan 1;136(1):31-81. doi: 10.1097/ALN.0000000000004002.
[24] Feldman JM, Hendrickx J, Kennedy RR. Carbon Dioxide Absorption During Inhalation Anesthesia: A Modern Practice. Anesth Analg. 2021 Apr 1;132(4):993-1002. doi: 10.1213/ANE.0000000000005137.