
The Anesthesia Gas Machine 2026
Michael P. Dosch PhD CRNA (ret), Darin Tharp CRNA MS
University of Detroit Mercy - Nurse Anesthesia
This site is https://healthprofessions.udmercy.edu/academics/na/agm/.
Revised Feb. 2026
The Anesthesia Gas Machine 2026
Michael P. Dosch PhD CRNA (ret), Darin Tharp CRNA MS
University of Detroit Mercy - Nurse Anesthesia
This site is https://healthprofessions.udmercy.edu/academics/na/agm/.
Revised Feb. 2026
The function of any breathing circuit is to deliver oxygen and anesthetic gases, and eliminate carbon dioxide. Carbon dioxide may be eliminated by either washout with adequate fresh gas flow (FGF), or by chemical absorption (soda lime).
Table below is based in part on Mapleson.[1].
|
Mode |
Reservoir (breathing bag) |
Rebreathing |
Example |
|
Open |
No |
No |
Open drop |
|
Semi-open |
Yes |
No |
NRB, or Circle at high FGF (> VE) |
|
Semi-closed |
Yes |
Yes, partial |
Circle at low FGF |
|
Closed |
Yes |
Yes, complete |
Circle (with pop-off valve [APL] closed) |
NRB = Non-rebreathing circuit (e.g. Mapleson D). VE = minute ventilation (RR x VT). FGF = Fresh gas flow.
|
Mapleson D. Click on the link to see the larger version.
|
|
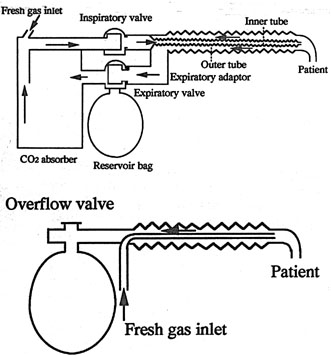
Mapleson D and Bain NRB circuit. Click on the link to see the larger version. The Bain circuit is a "coaxial" Mapleson D- the same components, but the fresh gas flow tubing is directed within the inspiratory limb, with fresh gas entering the circuit near the mask. Fresh gas flow requirements are similar to other NRB circuits. The Bain has been shown to add more heat and humidity to inhaled gases than other Mapleson circuits. |
|
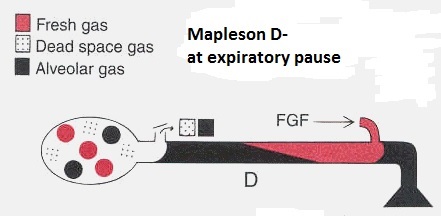
Mapleson D - how it works. Click on the link to see the larger version. How do NRB’s work? During expiration, FGF pushes exhaled gas down the expiratory limb, where it collects in the breathing bag and opens the expiratory valve (pop-off or APL). The next inspiration draws on the gas which is nearest in the expiratory limb (primarily FGF). The expiratory limb will have less carbon dioxide (less rebreathing) if FGF inflow is high, VT is low, and the duration of the expiratory pause is long (a long expiratory pause is desirable as exhaled gas will be flushed more thoroughly). All NRB circuits are convenient, lightweight, easily scavenged. One objection is that switching the breathing circuit back and forth between circle and Mapleson between cases introduces the possibility of misconnections. |
The Pethick Test for the Bain Circuit- A unique hazard of the use of the Bain circuit is occult disconnection or kinking of the inner, fresh gas delivery hose. If this occurs, the entire corrugated limb becomes dead space. This results in respiratory acidosis which is unresponsive to increased minute ventilation. To perform the Pethick test:
Dorsch & Dorsch give a second test.[2]. If fresh gas flow is established, and the inner tube is occluded, the flowmeter bobbins (if present) should dip (due to back pressure) if the inner tube is patent.
The circle is the most common breathing system. It cleanses carbon dioxide from the patient’s exhalations chemically, which allows rebreathing of all other exhaled gases (a unique breathing arrangement in health care, but rebreathing is used extensively in other environments e.g. space, submarine).
Good resources for understanding the circle and the role of each of their components are

|
Circle breathing circuit from Deranged Physiology: Breathing circuits for manual and mechanical ventilation. Click on the link to see the larger version. |

|
Circle system. Click on the link to see the larger version.
|
|
King circuit (top) compared to the Bain. Click on the link to see the larger version. A "Universal F" or "Mera F" circuit (KingTM circuit) is a coaxial circle system, with the inspiratory limb contained within the expiratory. Like a Bain, it is less bulky, and may offer more heat and humidification of the inspired gases. Like the Bain, occult disconnection or kinking of the inner limb causes a huge increase in dead space and respiratory acidosis.[3], [4]. . This respiratory acidosis does not respond to increased minute ventilation- if exhaled gases are not forced through the absorbent granules, no amount of ventilation will cleanse carbon dioxide from the patient's exhalations. The tests for inner tube patency which can be used for a Bain circuit are not readily adaptable to the King circuit. |

|
The Flow-i (and Mindray A9) use a volume reflector in the circle. Click on the link to see the larger version. |
Circle advantages:
Circle disadvantages:
[1] Mapleson WW. The elimination of rebreathing in various semi-closed anaesthetic systems. Br J Anaesth. 1954 Sep;26(5):323-32. doi: 10.1093/bja/26.5.323.
[2] Dorsch JA, Dorsch SE. Understanding Anesthesia Equipment 5th ed. 2008:942
[3] Nakae Y, Miyabe M, Sonoda H, Tamiya K, Namiki A. Comparison of the Jackson-Rees circuit, the pediatric circle, and the MERA F breathing system for pediatric anesthesia. Anesth Analg. 1996 Sep;83(3):488-92. doi: 10.1097/00000539-199609000-00008.
[4] Jellish WS, Nolan T, Kleinman B. Hypercapnia related to a faulty adult co-axial breathing circuit. Anesth Analg. 2001 Oct;93(4):973-4, table of contents. doi: 10.1097/00000539-200110000-00034.